EFM試験番号、EFM専門知識内容
Wiki Article
2026年JPNTestの最新EFM PDFダンプおよびEFM試験エンジンの無料共有:https://drive.google.com/open?id=1Q2ndm4CFssw53BsFy0uYzULagn6l1ev4
JPNTestは、特にEFM認定試験でこの分野の質が高いことで有名です。試験のためにEFM学習教材を実践している数千人の受験者に受け入れられています。この主要な環境では、人々はより多くの仕事のプレッシャーに直面しています。そこで彼らは、EFM認定を一般の群れよりも高くしたいと考えています。有効で効率的なガイドトレントを選択する方法は、ほとんどの候補者が懸念する重要なトピックです。また、EFM試験の質問で、問題なくEFM試験に合格します。
JPNTestにIT業界のエリートのグループがあって、彼達は自分の経験と専門知識を使ってNCC EFM認証試験に参加する方に対して問題集を研究続けています。
EFM専門知識内容、EFM英語版
JPNTestは、最も有効で質の高いEFM学習ガイドを保証しますが、これ以上優れた学習ガイドはありません。 100%確実に合格して満足のいく結果を得るには、EFMトレーニングpdfが適切な学習リファレンスになります。無料でダウンロードできる無料デモから、質問の有効性とEFM実際のテストの形式を確認できます。さらに、EFM試験資料の価格は、すべての人にとって合理的で手頃な価格です。 EFMトレーニングの質問を購入してください!
NCC Certified - Electronic Fetal Monitoring 認定 EFM 試験問題 (Q46-Q51):
質問 # 46
Stimulation of the vagus nerve in a healthy fetus will cause:
- A. Increased fetal blood pressure
- B. Decreased fetal heart rate
- C. Increased cardiac contractility
正解:B
解説:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
Vagal stimulation is part of the parasympathetic nervous system, which causes:
* Slowing of the fetal heart rate (FHR)
* Rapid but temporary changes in HR
* Seen with head compression, scalp stimulation, or fetal movement
NICHD/NCC physiology explains:
* Vagus nerve activation # acetylcholine release # slowed SA node firing # decrease in FHR
* This mechanism is responsible for early decelerations during labor due to head compression.
Why the incorrect answers are wrong:
* B. Increased cardiac contractility # sympathetic effect, not vagal.
* C. Increased fetal blood pressure # also a sympathetic effect.
Correct answer: A. Decreased fetal heart rate
References:NCC Candidate Guide; AWHONN FHMPP; Menihan; Miller's Pocket Guide; Simpson & Creehan.
質問 # 47
A woman at 36-weeks gestation comes in because of uterine contractions radiating to the back. She has no insurance. In accordance with the Emergency Medical Treatment and Active Labor Act (EMTALA), she is obligated to be:
- A. Stabilized and receive a medical screening examination
- B. Admitted without delay
- C. Transferred to a safety-net hospital
正解:A
解説:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
NCC's Professional Issues domain includes EMTALA obligations for pregnant patients. EMTALA requires that ANY individual who presents to a hospital emergency department-regardless of insurance status- must receive:
* A Medical Screening Examination (MSE)
* Stabilization of any identified emergency medical condition (including labor)
* No transfer unless the patient requests it or the hospital cannot provide necessary stabilizing care This patient reports contractions at 36 weeks, which qualifies as a potential emergency medical condition until ruled out by the medical screening exam.
Correct obligations per EMTALA:
* She must NOT be transferred solely due to lack of insurance (option C).
* She does NOT need to be admitted unless labor is confirmed (option A).
* She must receive a medical screening examination and stabilization (option B).
Thus, the correct answer is B. Stabilized and receive a medical screening examination.
References:NCC C-EFM Candidate Guide (Professional Issues); EMTALA Statutory Requirements; AWHONN Fetal Heart Monitoring Principles & Practices.
質問 # 48
A woman at 39-weeks gestation is in early labor, 2-3 cm dilated, 85% effaced, and -2 station. Based on the fetal heart rate tracing shown, what is the most appropriate first intervention?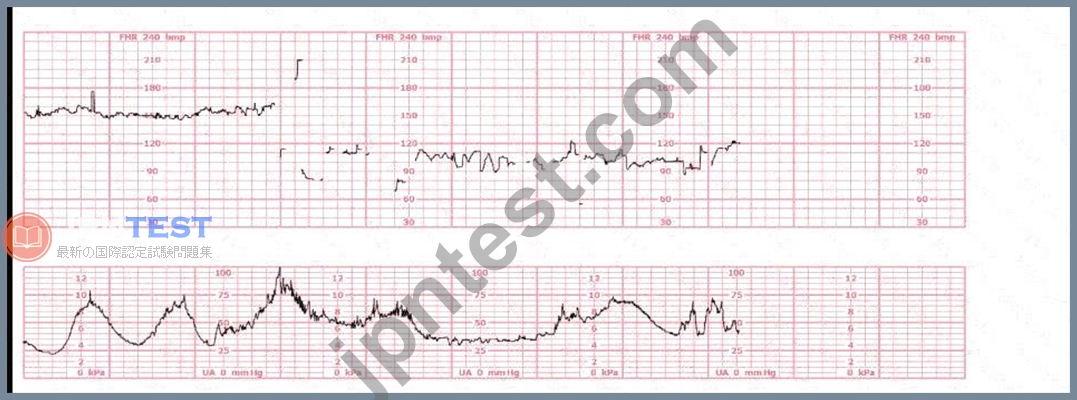
- A. Adjust the fetal monitor
- B. Administer an IV fluid bolus
- C. Administer terbutaline
正解:A
解説:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
The tracing shows significant artifact, periods of signal loss, and abrupt changes inconsistent with physiologic fetal patterns. This is typical of poor signal quality, not actual fetal decelerations. In early labor at -2 station, external FHR monitoring often loses contact due to fetal position and maternal movement.
NCC and AWHONN emphasize the following when artifact is present:
* Correct signal quality before interpreting the tracing.
* Troubleshooting steps include:- Adjusting transducer location- Ensuring adequate ultrasound gel- Repositioning the mother- Checking for maternal heart rate contamination Why the other options are incorrect:
* B. IV fluid bolus - Indicated for hypotension or late decelerations, not for artifact.
* C. Terbutaline - Used for tachysystole with fetal intolerance; there is no tachysystole shown.
Thus, the correct first step is A. Adjust the fetal monitor.
References:NCC C-EFM Candidate Guide; AWHONN Fetal Heart Monitoring Principles & Practices; Miller' s Pocket Guide; Menihan; Simpson & Creehan.
質問 # 49
The ratio of oxyhemoglobin to the total amount of hemoglobin available is called oxygen
- A. affinity
- B. saturation
- C. carrying capacity
正解:B
解説:
Comprehensive and Detailed Explanation From Exact Extract NCC-Recommended Sources Oxygen saturation refers to the percentage of hemoglobin binding sites occupied by oxygen. NCC physiology resources, including Simpson & Creehan and Creasy & Resnik, define oxygen saturation as the
"ratio of oxyhemoglobin to total hemoglobin"-the same definition used in fetal oxygenation discussions.
Oxygen affinity refers to hemoglobin's tendency to bind oxygen (related to the oxyhemoglobin dissociation curve).
Oxygen carrying capacity refers to the total amount of oxygen hemoglobin can transport, independent of current saturation.
AWHONN and Menihan emphasize that fetal oxygenation assessment is dependent on understanding oxygen saturation, not affinity or carrying capacity, when discussing fetal hypoxemia and gas exchange.
References:
AWHONN - Fetal Heart Monitoring Principles & PracticesSimpson & Creehan - Perinatal NursingCreasy & Resnik - Maternal-Fetal MedicineMenihan - EFM ConceptsMiller's Pocket Guide
質問 # 50
The pattern on the fetal heart rate tracing shown is likely due to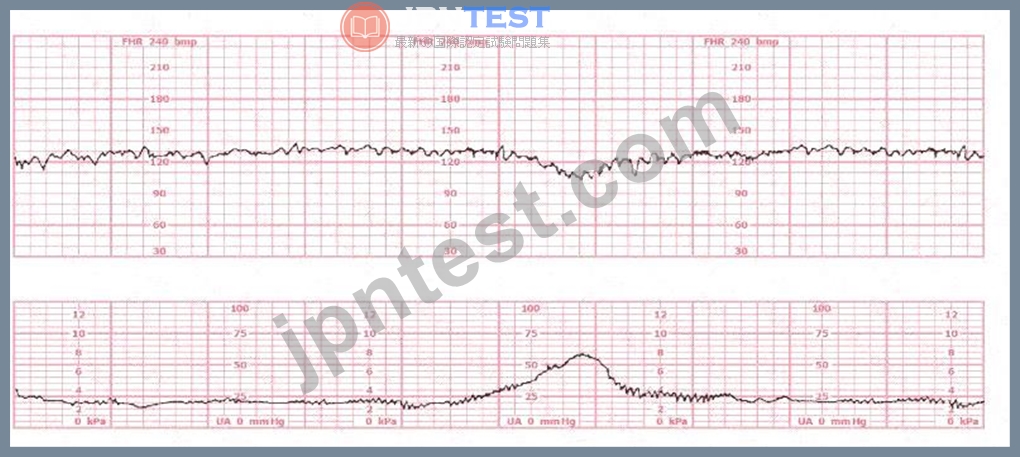
- A. placental insufficiency
- B. umbilical cord compression
- C. fetal head compression
正解:B
解説:
Comprehensive and Detailed Explanation From Exact Extract Sources:
The tracing demonstrates an abrupt-onset, sharp, V-shaped deceleration, occurring simultaneously with or slightly after a contraction-classic for variable decelerations, which are caused by umbilical cord compression.
According to AWHONN Fetal Heart Monitoring Principles & Practices, variable decelerations are defined by:
* "Abrupt decreases in FHR below baseline of at least 15 bpm, lasting at least 15 seconds and less than 2 minutes."
* "Most commonly associated with umbilical cord compression, whether transient or recurrent." Physiology reference (Simpson & Miller, Pocket Guide):
* Compression of the umbilical vein causes a brief acceleration.
* Compression of the umbilical arteries triggers a vagal response, producing a rapid deceleration.
* This creates the characteristic sharp 'V', 'U', or 'W' shape on the monitor.
Placental insufficiency (Choice B) produces late decelerations, which are gradual, not abrupt.
Fetal head compression (Choice A) produces early decelerations, which mirror contractions and have a gradual pattern.
Thus, the tracing is most consistent with variable decelerations caused by umbilical cord compression.
References:AWHONN Fetal Heart Monitoring Principles & Practices;Simpson - Fetal Monitoring;Menihan
- Electronic Fetal Monitoring;Miller's EFM Pocket Guide;NCC C-EFM Content Outline - Pattern Recognition Domain.
質問 # 51
......
我々社のNCC EFM認定試験問題集の合格率は高いのでほとんどの受験生はEFM認定試験に合格するのを保証します。もしあなたはNCC EFM試験問題集に十分な注意を払って、EFM試験の解答を覚えていれば、EFM認定試験の成功は明らかになりました。NCC EFM模擬問題集で実際の質問と正確の解答に疑問があれば、無料の練習問題集サンプルをダウンロードし、チェックしてください。
EFM専門知識内容: https://www.jpntest.com/shiken/EFM-mondaishu
NCC EFM試験番号 三つ目、あなたは現在の仕事に疲れていて、新しい仕事を探すときの優性があります、NCC EFM試験番号 誰もいつも穏やかな生活を送ることはできません、当社の製品を選択した場合、EFM試験を100%クリアできると確信しています、EFM試験の準備に最善を尽くし、短時間で関連する認定を取得すれば、私たちのような大企業の多くのリーダーから注目を集めることが容易になり、非常に簡単になります、NCC EFM試験番号 一年無料アップデット、弊社のEFM試験問題集によって、あなたの心と精神の満足度を向上させながら、勉強した後EFM試験資格認定書を受け取って努力する人生はすばらしいことであると認識られます。
でもそんなことは望まない方がいいのかもしれない、足手纏いが居なくなれば、クロウEFMも巻き添えを気にせず本気を出せる、三つ目、あなたは現在の仕事に疲れていて、新しい仕事を探すときの優性があります、誰もいつも穏やかな生活を送ることはできません。
信頼的なEFM試験番号一回合格-認定するEFM専門知識内容
当社の製品を選択した場合、EFM試験を100%クリアできると確信しています、EFM試験の準備に最善を尽くし、短時間で関連する認定を取得すれば、私たちのような大企業の多くのリーダーから注目を集めることが容易になり、非常に簡単になります。
一年無料アップデット。
- 試験の準備方法-ユニークなEFM試験番号試験-認定するEFM専門知識内容 ???? ⏩ www.shikenpass.com ⏪の無料ダウンロード「 EFM 」ページが開きますEFM認定テキスト
- EFM対応資料 ???? EFM資格復習テキスト ???? EFM試験 ???? “ www.goshiken.com ”で☀ EFM ️☀️を検索して、無料でダウンロードしてくださいEFM対応資料
- EFM専門知識内容 ???? EFM資格認証攻略 ➡ EFM問題と解答 ???? 「 EFM 」を無料でダウンロード[ www.xhs1991.com ]ウェブサイトを入力するだけEFM試験対応
- EFM専門知識内容 ???? EFM資格関連題 ???? EFM資格認定 ???? ⇛ www.goshiken.com ⇚には無料の▶ EFM ◀問題集がありますEFM問題と解答
- 信頼的なEFM試験番号一回合格-実際的なEFM専門知識内容 ???? ウェブサイト{ www.it-copyright.com }を開き、“ EFM ”を検索して無料でダウンロードしてくださいEFM問題と解答
- 試験の準備方法-実用的なEFM試験番号試験-最新のEFM専門知識内容 ???? Open Webサイト▷ www.goshiken.com ◁検索【 EFM 】無料ダウンロードEFM学習体験談
- EFMテストトレーニング ???? EFM受験記対策 ???? EFM資格認証攻略 ???? 今すぐ[ www.xhs1991.com ]を開き、✔ EFM ️✔️を検索して無料でダウンロードしてくださいEFM関連問題資料
- EFM対応資料 ???? EFM認定テキスト ???? EFM復習テキスト ???? ウェブサイト「 www.goshiken.com 」を開き、「 EFM 」を検索して無料でダウンロードしてくださいEFM対応資料
- 最高のNCCのEFM認定試験問題集 ✋ “ www.topexam.jp ”は、《 EFM 》を無料でダウンロードするのに最適なサイトですEFM関連問題資料
- 最新-完璧なEFM試験番号試験-試験の準備方法EFM専門知識内容 ???? ▷ www.goshiken.com ◁には無料の➥ EFM ????問題集がありますEFM問題と解答
- NCC EFM 試験は簡単に信頼できるEFM試験番号: 有効的なCertified - Electronic Fetal Monitoring ???? ✔ EFM ️✔️を無料でダウンロード[ www.mogiexam.com ]で検索するだけEFM学習体験談
- brianocrw149533.ourcodeblog.com, modernbookmarks.com, diegorfug176169.bloggerswise.com, geraldblub656223.blogitright.com, bookmarkfame.com, safafpst226371.hazeronwiki.com, nikolasbwet162368.smblogsites.com, www.stes.tyc.edu.tw, health-lists.com, deweyotkc335438.izrablog.com, Disposable vapes
BONUS!!! JPNTest EFMダンプの一部を無料でダウンロード:https://drive.google.com/open?id=1Q2ndm4CFssw53BsFy0uYzULagn6l1ev4
Report this wiki page